By Prim. Dr. Tome Tasevski
This is a very interesting topic, 3D CBCT. Why? Because, there are many dentists that do implants or other surgical treatments, but they do not use this very significant diagnostic image. They just do 2D panoramic x-ray images or maybe in some cases just intraoral x-ray images. Now, YOU will ask: Why? Well, my dear readers, I am asking the same question. Why?
At the beginning of my practice as an implatologist, I also did not use it, but not because I did not need it. Simply because I couldn’t, i.e. there was not available such kind of equipment in my country. So, very short after I began implanting I bought the necessary 3D CBCT and from that point after, it is my first move when I do implants.
Why do we take panoramic images or OPG?
Panoramic imaging is a standard procedure to survey the whole dental status. In panoramic imaging the patient’s jaws and facial bones are scanned with a narrow x-ray beam, which rotates around the patient producing a sharp image layer.
A panoramic image shows a curved layer of the jaws, including temporomandibular joints (TMJ). It is considered to be the starting point of most treatments and imaging tasks.
Panoramic x-ray devices produce a wide range of two-dimensional clinical views, e.g. adult pan, paediatric pan, TMJs, segments (partial panoramic view of a selected region in the dentition), sinuses, bitewing.
Panoramic images are valuable diagnostic tools, for example in these clinical tasks:
- Overall condition of the dentition and TMJ’s
- Detecting:
◦ impacted or supernumerary teeth
◦ large pathologic lesions in the jaws
◦ abnormalities in adjacent structures such as the maxillary sinuses
◦ advanced periodontal disease
- Preliminary assessment of implants
Benefits of panoramic imaging
- Fast way to obtain image of entire dentition (compared to intraoral)
- Low radiation dose compared to size of anatomy covered
So, what is the limitation of OPG or 2D radiograph in implant dentistry?
Using the 2D or OPG radiograph in the treatment plane of implant placement is with great limitation in defining the exact location of the anatomical structure. This will make the operator to experience:
- The worse situation, this occur when it is difficult to determine the exact location of inferior dental nerve, the operator will choose the nearest to the alveolar ridge and consider it as the location of the nerve, to avoid inferior dental complex damages;
- Short diameter implant to avoid jeopardizing the vital structure;
- Narrow diameter implant, difficult to estimate the width of the alveolar ridge or edentulous area apically and coronaly, thereby making the operator to choose narrow implant in order to be in the safe side;
- Open and see technique, whether the ridge needs bone augmentation, expansion or implant angulations;
- Under or over estimation of the bone density, operator will totally depend on the hand sensation during osteotomy procedure to determine the bone density or quality;
- Unaware about any anatomical variation, like mandibular incisive canal, anterior loop of inferior dental canal and mental foramen location;
- In upper anterior immediate implantation, buccal (frontal wall) bone width is crucial in determining the treatment plane, whether immediate implant can be proceed after tooth extraction or socket augmentation and delay implant placement is better?
All this information is difficult to extract from 2D images.
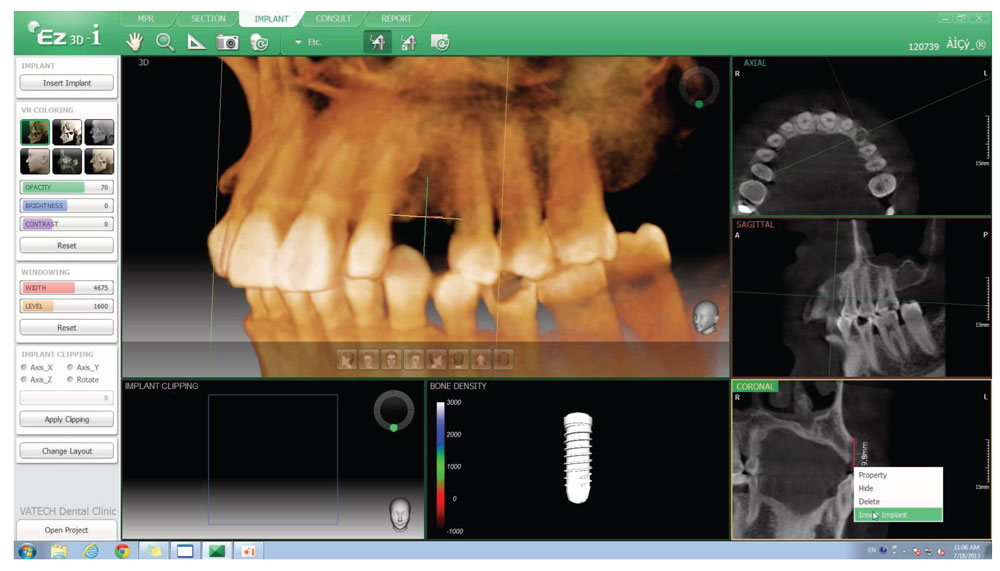
So, there is no doubt that 3D images give big advantages for dental implantologist and patients with superiority compare to 2D images. Transfer of treatment plane into successful treatment is more achievable with 3D images. It takes into consideration less complication, no time wasting for dentist and patient, no financial loss for both patient and the dentist. However, it also builds up the confident between the dentist and the patient, and more trust in dental implant as one of treatment option for the patient.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}