By Dr. Riste Panajotu
Implantology is a very exciting science.More exciting than the implantology is “Implantology in the frontal visible part of the mouth”.
Replacing a single frontal tooth with implant is a chalenge for every dentist, implantologist, periodontologist, oral surgeon etc.Its simply chalenging!
Imediate implantation – the most common technicque which is used in order to achive ridge preservation and bone volume preservation after tooth extraction.
Risk of losing vestibular bone height and respectively soft tissue is unacceptable from aesthetic point of view.
The literature reports that we can expect to have a recesion on the buccal gingiva after imediate implant placing at least 1mm and more in thin gingival biotypes( Howard Gluckman).
There are some studies witch are prooving that an overall reduction in the horizontal dimensions occurred following tooth extraction and that the resorption of the buccal part of the ridge was more pronounced than the lingual one.
It is well known that physiology processes taking place immediately after tooth extraction, including increased number of osteoclasts on the outside and inside buccal and lingual bone walls.
The presence of osteoclasts on the inner surface of the socket walls indicates that the bundle bone, which is closely related with the periodontal tissue is going to be resorbed. Anatomically buccal bone of the teeth is thinner than lingual or palatal one. There for as bundle bone is tooth-dependent tissue it will gradually disappear after extraction.
So since there is more bundle bone in the crest of the buccal than the lingual wall, hard tissue loss will become most pronounced in the buccal wall (Lindhe, Clinical periodontology and implant dentistry, 2008)
These scientific evidences and the clinical experience of immediate implant placement in fresh extraction sockets have led us think that probably by preserving the periodontal tissues on the buccal part of the socket we could prevent bone resorption in this critical area.
Also in order to prevent the horizontal and vertical bone loss after extraction we use various methods of guided bone regeneration(GBR) like filler materials and membranes , to support the bucal plate and soft tissue ,to stabilize the coagulum and prevent epithelial ingrowth.
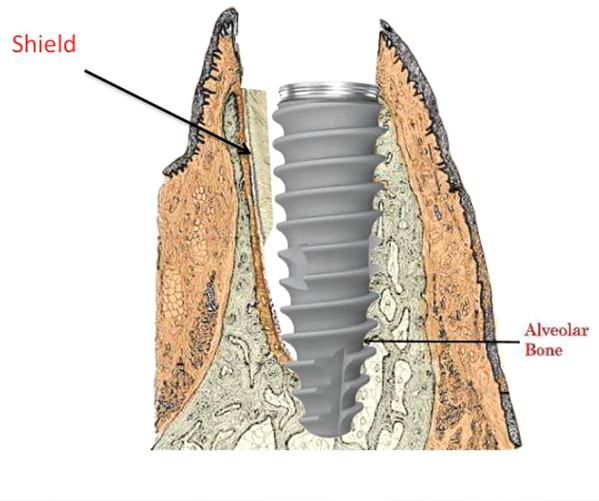
The socket-shield (SS) technique provides a promising treatment and better managing these risks and preserve the post-extraction tissues in aesthetically challenging cases.We need to preserve and use in our advantage the Bundle bone.
The principle is to prepare the root of a tooth indicated for extraction in such a manner that the buccal / facial root section remains in-situ with its physiologic relation to the buccal plate intact. The tooth root section’s periodontal attachment (periodontal ligament (PDL), attachment fibers, vascularization, root cementum, bundle bone, alveolar bone) is intended to remain vital and undamaged so as to prevent the expected post-extraction socket remodeling and to support the buccal / facial tissues. (Howard Gluckman,1 Jonathan Du Toit,2 Maurice Salama3)
How to do this practicaly:
1.Cut the crown of the tooth which is going to be extracted
2.Section the root (separation) in the mesiodistal direction as far apical as posible using a long apropriate bur.
3.Now the root is separated in facial and palatal/lingval section.Extract the palatal/lingval portion gently and leave the facial part attached to the tooth socket.
4.Reduce coronally the remaning root section to 1mm above alveolar ridge and ensure a concave atraumatic conture of the shield
5. The tooth socket’s palatal wall and apex were then curetted to remove any tissue or infective remnants and the root section was checked for immobility.
6.Prepare the site for implantation and then put the implant palatal of the socket shield



{kind=link}
{kind=link}
{kind=link}