
Prim. Dr. Tome Tasevski
I’ve always loved the concept of minimally invasive, i.e. atraumatic approach for everything about dentistry. I’ve never respected the learning of wide opening of cavities, preparation of teeth more than needed, endodontics with wide crown openings, surgical opening flaps etc. Why do we that? Old knowledge says that in order to approach the problem, you have to open wide and look at it thoroughly. Yes, it is like this, but today we have many tools and technology that we can use, in order not to make this kind of trauma either to teeth, gums or alveolar bone. My experience taught me that the bigger trauma you make the bigger problems you get! First for the healing process, second for the patient in general and third for you. You never want that!
And what is Minimally Invasive/Atraumatic Immediate Implantology or in short AII?
It is my new approach in immediate implantology, new concept where we don’t use any scalpel, we do not create any opening flaps or do bone leveling and we do not use any sutures. It is a concept where we use the dental alveola as an implant alveola or how other like to call it implant site, and as for hemorrhage we rely on biologic hemostasis.
As all treatments, in order AII to be applied, we must have certain indications, which are as follows:
- Patient has to be in good general health, especially to be excluded from the systemic diseases like hemophilia, osteoporosis, diabetes or whatever cardio pathology factors;
- 3D CBCT is essential;
- Teeth that would be extracted has to be indicated for extraction;
- We must have more teeth with roots into the alveolar bone at least 1/3 or less from bone level;
- We need more teeth or remained teeth have to be adequate to our implant positioning plan – all on 4 or all on 6, mobile or fixed prosthetics;
- The alveolar bone has to have good height and width, especially at upper and lower molar region;
- BQI is important but not necessary ;
- Patient MUST be very well informed and managed before and after the treatment regarding the procedure, especially post op because of great hygiene needed;
- Several post op check ups.
Now, please watch the video very carefully:
As you can see in the video, first we must have good analytics of the patient examination and of course a treatment plan. You saw that more of the teeth were extracted with the fingers, which means that whatever therapy we’ve made it would only be a delay to the treatment. When finished with extraction, the most important that we must do is a good curettage and cleaning of the debris (manually or mechanically). Clinical measurement are more than needed at any time of the treatment. The first probe you see is a surgical probe and with it we measure the depth of the implant alveola. The second probe is periodontal probe and measurements are made in order to ensure the exact highest point of the alveolar bone (below papilla). In that way, we immediately know where we are, if we need any adjustments to the treatment plan made, we comply to it or we modify it.
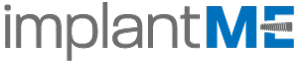
After the drilling (according to brand implant protocol) we immediately place the dental implants, which for this case were dm4,20 and height 13mm, and we screw the most suitable healing caps. The implants were placed with force of 50Ncm. This force does not mean anything, please read my text https://implantme.com/primary-implant-stability-myth-or-reality/ so that you will get a clear picture. You do not need any sutures because you rely on the biologic hemostatic functions.
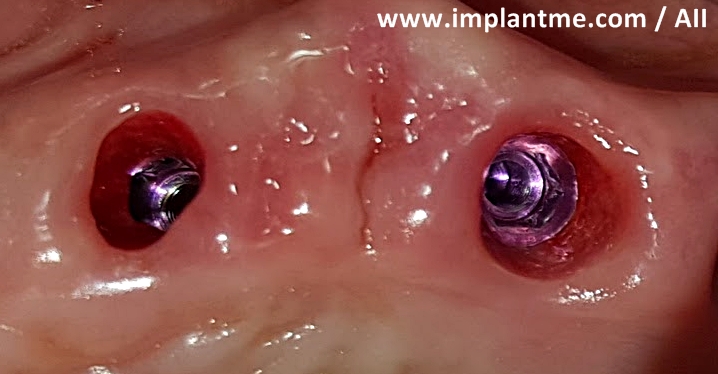
The treatment was finished in approximate 20-25 minutes, which is very important for the patient. Here is the photo after the treatment (x-ray and clinical):

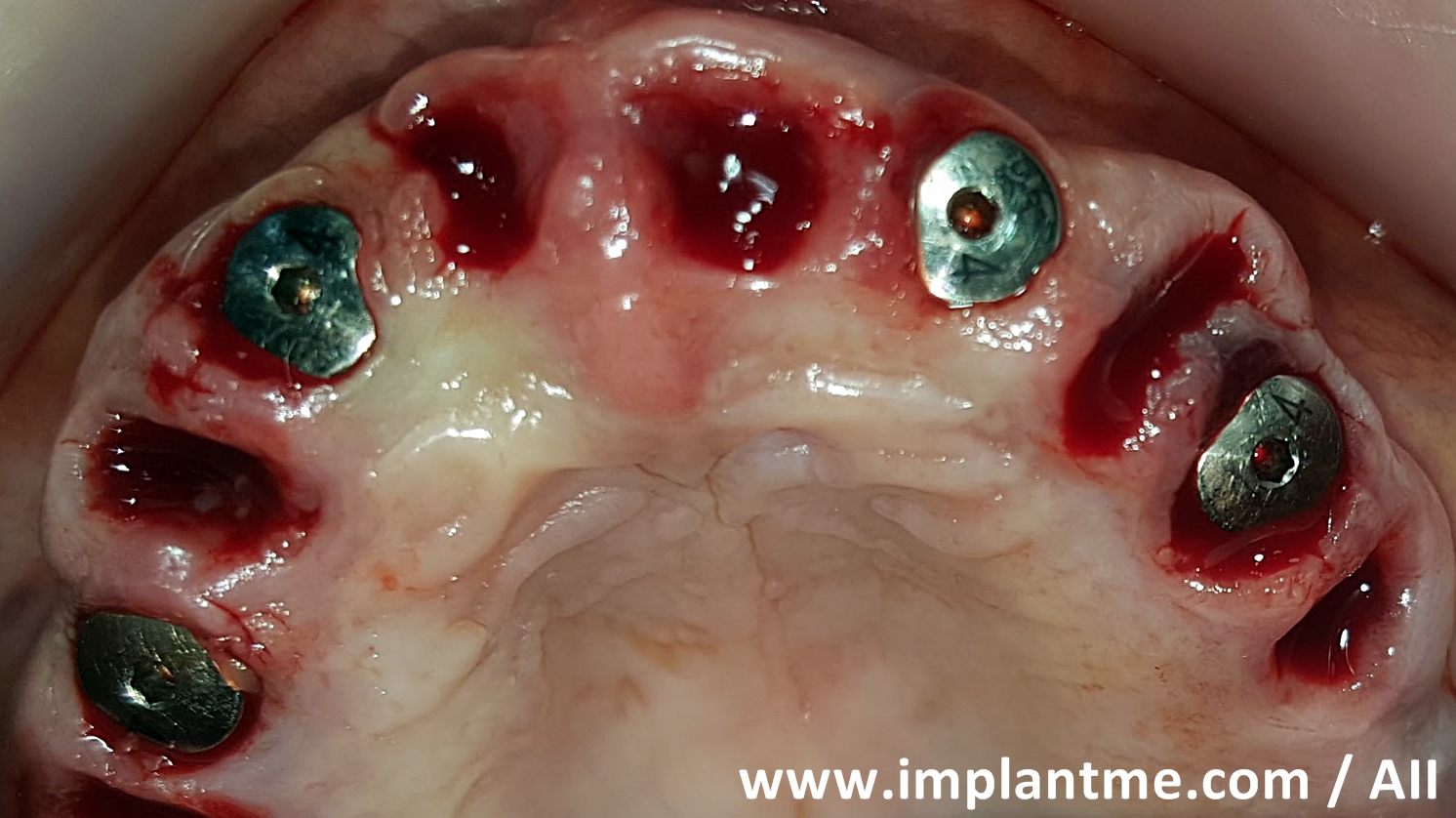
Here, after 1 week:

And, what do you see? YES, amazing healing! The dental alveola is closed, gingiva is with a great color and the most important for us, we have great implant sulcus!
Here is a photo after 4 weeks:


And here is after 2 months:


As you can see very small intraoral difference is present. The bone level remains the same as the start post op x-ray.
So, what can we say for AII?
- The treatment is very short time consuming for the patient;
- The extraction of the teeth and the good curettage made clean and sticky blood to be present, which is very important for the osseontegration of the implant (please read my text https://implantme.com/no-blood-no-connection/ so you will know why this is very important)
- Socket shield is ensured;
- Gingiva healing is ensured;
- Implant sulcus is ensured;
- Crown saddle are present by post op day 1 or will be more easily applied.
Conclusion: for me AII is the best approach, of course if you have the indications. It is up to YOU either to accept it or to hold with the old school. Maybe you will use surgical guides or you will make the wide surgical openings in order to play more safe. However, at the end of our working day, I hope, we all wish the same – the best for our patient!




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}